
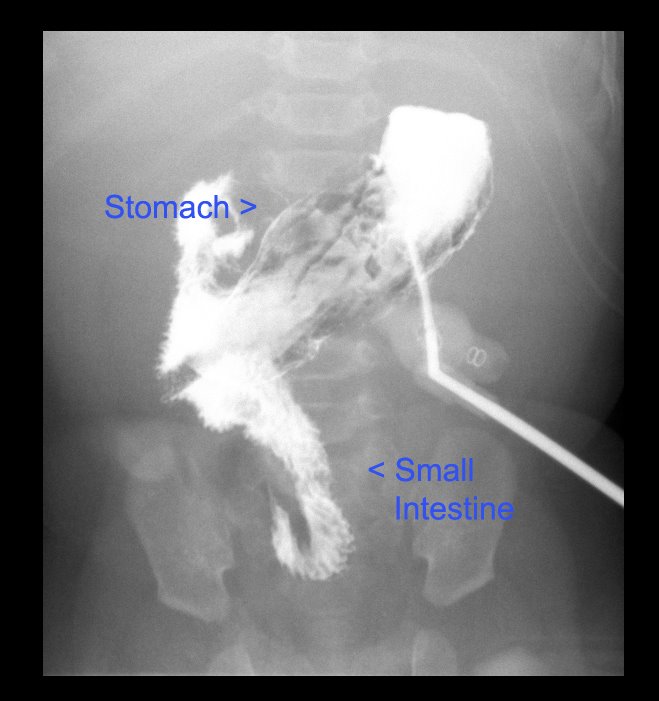
We had Patrick’s g-tube study done. (Great results! Nothing wrong. Just a slightly upward angle that makes positioning the tube tricky.) As part of the history, they asked when the gastrostomy (g-tube hole) was created and I realized last night that I could have answered “exactly two years ago.”
Why do I remember that? Well, because exactly two years ago yesterday, the court officially named us as Patrick’s legal guardians. It was the best birthday present I’ve ever gotten.
A friend of mine has been doing something special this month on her blog. Because it’s national adoption awareness month, she’s been posting daily adoption related posts. She invited me to be a guest blogger and, by coincidence, will be running my post today… a very significant 2 year adoption anniversary for us.
So, I thought I’d share with you what I wrote for her. Here goes:
————————————————————————–

Ours is not a typical adoption story, because Patrick is not a typical little boy. His life was meant to be something different, something miraculous, and so it required that it start in a very different and miraculous way.
But my part of the story starts the way a lot of others do. We wanted to have children. When that didn’t happen easily, we involved doctors. For years, we went through the ups and downs of charting and temperature taking, tests and medications. Finally, after several years and a minor surgery, our doctor sat us down for “the talk.” He explained that there were several causes of my infertility. The cards were, essentially, stacked against us. He still felt it very possible that we could have children, but only with major medical intervention. We had some big choices to make.
We talked about it and we prayed about it. And then, that Sunday, as we sat in church, we received a clear answer that it was time for us to stop medical treatments. Our child would come to us through adoption.
With a path finally before us, we moved forward quickly. I’ve never felt so driven to do anything before in my life. In under a month, we completed the application process, training classes, and were mostly done with our home study.
During our home visit, we had a conversation with our case worker that would play a major part in bringing Patrick into our family. She’d looked at our “preferences checklist” and noted that we seemed more open than most to adopting a child with special needs. We explained that we felt that adoption was a faith process. We believe that Heavenly Father puts families together. We knew we’d never turn away a child born to us with medical problems. So, if God was in charge of adoptions, too, then why would we limit His options? We knew Heavenly Father would help us find our child and that, if the child really belonged in our family, race and health wouldn’t stand in the way.
We decided to adopt in June. Our application was approved in September and we hunkered down for a nice long wait. We figured two years, at the least, was the average we’d heard. And still, by the end of October it felt like far too long. My heart ached for a child it knew was missing.
Then, on a very snowy morning the first week of November, my phone rang. It was my case worker. She started out by saying, “There was a little boy born on Halloween in Michigan.” My heart skipped a beat. I grabbed a pen and a piece of paper and started scribbling notes. She told me he was Korean. And then, she went on to tell me that he’d had a birth defect. His intestines had developed on the outside of his abdomen. The doctors were saying he had a life expectancy of 1 to 2 years. They needed to find an adoptive home quickly because doctors wanted to discharge him from the hospital. All she could tell me about his family that his birth mother wanted him to be able to go to the temple to be sealed to a family.
She said she’d send an e-mail with more information and a picture. She encouraged me to talk to Brian and decide if we’d like to be among those families considered to adopt this little boy, and then to call her and let her know.

As soon as I gathered myself, I called Brian. But he wasn’t at his desk. Meanwhile, two e-mails arrived. One was a short paragraph from the baby’s caseworker in Michigan explaining his medical needs and the unconventional and hurried search for parents. In the other were two photographs of a sweet little Korean boy with great big eyes and an IV in his head.
Since Brian wasn’t at his desk, I called the insurance company to find out if this we even had coverage to pay for this kind of medical problem.
That’s how Brian first found out about the offer. While I was on hold with the insurance company, he called back on my cell phone, so he heard me finish the conversation about “preexisting conditions” and “adoption”.
I gave Brian the information and, after a quick moment of thought, he said he’d come right home.
We had a prayer together, then went to the temple – the perfect setting to make decisions about life and death and eternity.
I knew that families are eternal. I knew that mortality is not the end of life. And yet, I was filled with grief. It was as if I’d just been told I was carrying a child with a terminal illness, but he wasn’t even mine yet. And I was scared. I didn’t know if I was ready to leave the life I knew then.. abandon it all, and become mom to a child who would need so much help, and who had such an uncertain future.
Still, when Brian turned to me and said, “I think we should pursue this,” my heart leapt with joy.
So, we called our caseworker and gave her a list of questions we had. And then we went to visit our parents. We felt we should tell them about the offer, because we knew that whatever happened, we were never going to be the same. And we both wanted father’s blessings. We showed them the little boy with the angel eyes and explained that we didn’t know if he was ours.. But from that moment, all of our families were praying for a little boy whom the e-mail called “Patrick.”
That was Wednesday. Thursday, I sent a copy of our profile. Friday afternoon, as I on my lunch break with Brian, our case worker called my cell phone. The birth family had seen our profile and had chosen us to adopt their baby.
Now, we had a choice to make. Because we’d been selected, we could finally start filling in the gaps in the medical information we were getting. And boy, where there gaps! We called the baby’s caseworker, who referred us to the hospital social worker. Finally, we decided we needed to talk to doctors, and we needed to do it face to face.
I called my mom and told her to take my credit card and buy airplane tickets. Then, I went back to work, explained what had happened, and asked for a leave of absence. After that, we went to the adoption agency where we signed pre-placement paperwork required for us see the baby in the hospital.
Friday night, we tried to get ready. We booked a long-term stay hotel room. We faxed legal documents to Michigan. We make a shopping list of nursery items. And we tried to pack.
I packed my bags that night not knowing what exactly I was packing for. We still didn’t know enough to say if we could take care of this baby. We didn’t know if or when he’d be discharged. We didn’t know how long it would take before we’d be given permission to leave the state again.
And yet, Saturday morning as I sat on a plane to Detroit, 10 rows ahead of my husband, I felt a quiet, happy calm. If nothing else, I knew it would be ok.

We met Patrick, his family, and his doctor Saturday night. It wasn’t what we expected. Due to unforeseen problems, things were tense at the hospital when we arrived. We felt like we knew nothing at all about his condition when we heard the doctor’s account. His case was much more severe than we’d understood, but the immediate prognosis was better.
At last, they led us to his room. My first impression was of how small he was. He was SO tiny! Just a little ball with wires and tubes attached. Without them, you’d have never guessed there was anything wrong.
They let me hold him while we talked. He felt so small and fragile.
I thought that the moment I met my baby, or the moment I held him, that I’d know he was mine. But that isn’t what happened for me. There were too many questions, still and I’d have to wait for that confirmation.
Sunday, we arranged to spend the day with Patrick. The nurses were so kind to let us change his diapers and help with other aspects of his care. I sat for hours singing him lullabies and watching monitors and letting him sleep.
When we arrived, the nurses warned us that he had a reputation as a very irritable little boy. There was even a sign on his door warning not to wake him. He was famous for screaming hysterically if his sleep was interrupted. But that’s not the baby I met. He was just a sweet, tiny little boy who wanted to be held.
I remember singing to him: “I am a child of God, and he has sent me here. Has given me an earthly home with parents kind and dear.” And my voice choked on the words because I knew that right at that moment, Patrick didn’t have that. I couldn’t imagine how any little boy could go through all he’d need to go through alone.
That night, as we looked at pictures from the day, I came across one that showed just his face with a white background. I knew, when I saw that picture, that I loved him.. and I wanted to keep him.
Monday morning, we held a “family conference.” It was a business day so we finally had been able to confirm that there were doctors to take care of him at our hospital at home. Our insurance confirmed that he’d be covered. Brian needed to hop on a plane to go back to work. (He was running a conference that week.) So, knowing we had the resources to provide for his physical needs, we asked Patrick if he’d like to be a part of our family. I swear, he looked up at Brian and smiled.

The case worker rushed to the hospital and by 1, we’d signed paperwork, and I was on my way to the airport with my husband. I was staying behind to start a whole new life.
The next few weeks in Michigan are among the sweetest of my life. With nothing else to do but hold my new baby and learn to care for him, I virtually lived in the NICU. My mom came for a week and shared with me in Patrick’s first feeding, first bath, and first time wearing real clothes. This time was also some of the hardest I’d experienced as I received a trial by fire as a mom of a child with major health problems. Patrick had his second surgery the day Brian flew back to be with us.

Two weeks after we signed papers, on my birthday, the birth parents appeared in court, and we were named as Patrick’s legal guardians. A week later, we had permission to bring him home. At 4 a.m. Thanksgiving day, Patrick and I arrived at Primary Children’s Hospital by air ambulance. He’d spend the next few weeks there as the doctors here got to know him and made arrangements for us to take care of him at home.
Because of his medical needs, the courts granted an early finalization of his adoption and we were able to take Patrick to the temple to be sealed as a forever family in February when he was just 4 months old.

Patrick just turned 2. He is an active, happy toddler who loves cars and music and Elmo. He is a living miracle! Patrick’s birth defect came with a rare complication. As a result, at birth he was missing over 95% of his small intestine. Without intestine, he doesn’t get nutrition by eating. In fact, eating large amounts puts him at risk for dehydration and bowel obstruction. Instead, he is entirely dependent on a form of IV nutrition called TPN. He has a permanent IV tunneled through his chest, into a vein in his chest or neck that runs to his heart.
The TPN leads to complications like infection and liver disease. In his short 2 years of life he has already struggled with both. Patrick’s doctors warned us before we adopted him that we’d become such regulars in the E.R. that we’d be on a first name basis with the staff. We soon found that to be true not just for the E.R. staff, but also the IV team, the infectious disease team, the PICU team, most of the residents, several of the medical students, and the entire gastroenterology department.
At 9 months old, as a result of infection, Patrick’s heart stopped. The fact that he is alive now is nothing short of a miracle. No doctor who hears his story and then meets him can help but confess that he has beaten the odds in countless ways.
Patrick will eventually need an intestinal transplant. He is already running out of places to put new IV’s and each new infection makes him a little more fragile.
Since they don’t do intestinal transplants where we live, we have chosen to have Patrick listed at Seattle Children’s Hospital. Patrick has been on the waiting list since April of 2009. He is status 1A and will have his transplant is soon as a donor match is found.
People try to tell us sometimes what a tremendous thing we did in adopting Patrick. We don’t really feel it’s something we can take credit for. As we told our caseworker when this all started, Heavenly Father puts families together. He knew Patrick needed us. And what’s more, He knew we needed Patrick.
Raising Patrick has taught us more about life than any other experience. We have learned to rely entirely on the Lord. We have learned to live each moment to it’s fullest. We have learned to lean on one another when things are hard and we to trust in hands of friends and strangers when we felt too weak to stand on our own. And we have learned to love like we didn’t know it was possible to love.
























{kind=link}