We’ve been a very busy little family lately. Patrick is 5 months old now. And in the time since I last posted, we’ve had a lot of firsts. So, here are some highlights.
 First giggles
First giggles
Patrick learned to laugh a while ago, but we didn’t get out and out chuckles until we discovered that the kid who used to scream his head off whenever he got undressed is ticklish and loves to have his clothes off. Dressing and especially weighing are now favorite games… but it’s best when daddy just picks him up without clothes on and tickles his back.
Today we learned that you can also get belly laughs if you squish his cheeks.
 First fever
First fever
Well, it all started with a cold, that turned into croup. After a week and a half trying to fight it off, Patrick got his first fever. Fortunately, it didn’t go much higher than 100.4 (38 degrees Celsius) and so we were able to have blood cultures drawn at home and his fever was gone in a day. No infection, thankfully. Just a day at home with Mom holding Patrick and taking his temperature every half an hour to make sure it hadn’t hit the danger mark yet.
 First necktie
First necktie
My brother Steven got married at the end of March. Although we were crazy busy working on his wedding cake and pictures, I just couldn’t help taking the opportunity to make Patrick and Brian matching neckties. We bought a tie with a matching handkerchief. Patrick thought his tie was a great toy to hold and chew on.
Oh, and a disclaimer on this picture. Patrick hates bright lights of any kind and we had studio lights on. Someday we’ll get a family picture with him not crying.
First rollover
I set Patrick down and turned my back on him for just a minute. When I turned back, he was on his tummy looking up at me as if to say “Whoa, Mom! What do I do now?” So far no signs of him having any idea how he did this or how to do it again. But we’re having much more play time on the floor to encourage him.


First haircut
After weeks of trying, we finally got time to take Patrick to my Grandpa’s house for his first haircut. In my defense (for those of you who thought I should never cut it), his hair was in his eyes and under his chin. Patrick was ok with the whole haircut idea till we hit the ticklish spot behind his ears. Finally, though, he fell asleep and we were able to finish. It’s a nice short cut.. but we hope that means it can grow for a while again before it needs another cut.
First ER visit
Last Saturday night, I noticed some bleeding under the dressing for Patrick’s central line. The line had shifted and, on closer inspection, we found that it had been pulled. It didn’t pull out, but was far enough to worry us. So – we got to make our first trip to the ER.
We were probably quite the sight there because, unlike the other families, we weren’t panicked. Central line issues are just part of life with Patrick. We’ve been planning and practicing for this trip for a while.
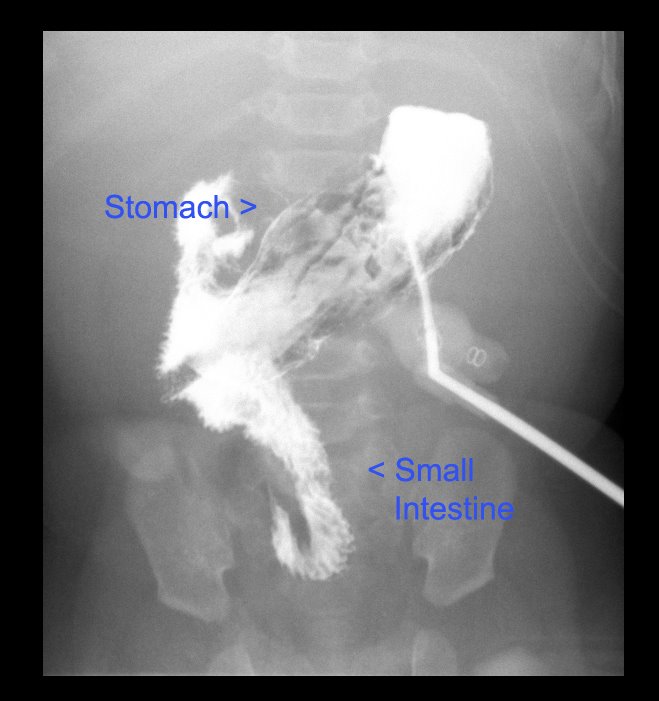
We arrived at 10:30 p.m. and had a bit of a wait in the waiting room because we were definitely not the most urgent case there. They took some x-rays to see the position of the line and about 1 a.m. the surgeon who placed Patrick’s line came into the room. He had been called in for an emergency appendectomy, and stopped in to see Patrick while he was there. He looked at it and said that the line was in a good position and he didn’t think it needed to be replaced on an emergency basis. Instead, we were to put antibacterial ointment on it twice a day to prevent infection, which meant lots of dressing changes, and then get a second opinion on Monday.
We were amazed, but happy, and after teaching an E.R. nurse proper technique for dressing change (yes, us teaching her), we were sent home. We got home at 3:30 a.m., connected Patrick’s feeding tube, and slept in till 11:30 a.m.
 First outpatient surgery
First outpatient surgery
So that brings us to Monday. About a month and a half ago we started the battle of the granulation tissue. Patrick had a patch of it next to his stoma that just kept growing back, no matter what we did. We learned to use silver nitrate to treat it, but it just kept coming back. So – we decided that maybe it was doing no harm and we’d leave it as it was.
No sooner had we made that decision than I discovered that his g-tube was surrounded by granulation tissue. A visit with the nurse practitioner in the GI clinic taught me better technique for nitrate treatments and after 10 miserable days of treatments, his G-tube site was clear of it. However, the spot by his stoma was starting to make it hard to keep a bag on and his skin was getting sorer by the day. I tried my newly practiced skills, but the tissue just kept coming back
So, we called and scheduled an appointment to have it electrocauterized. This is a minor procedure, but it’s painful and so they put babies to under so they don’t have to suffer through it. The surgeon we saw in the E.R. told us to as for follow-up at our appointment on Monday. It was still looking sore and red and swollen and the surgeon didn’t like the look of it, so he decided it was best to change the central line.
 This means that they took it out of one vein and put it into another one, coming out in a different place on his chest. Again, this is something we’d been warned about, so it wasn’t a complete shock. However, we were a bit nervous and, after an already long weekend, quite tired.
This means that they took it out of one vein and put it into another one, coming out in a different place on his chest. Again, this is something we’d been warned about, so it wasn’t a complete shock. However, we were a bit nervous and, after an already long weekend, quite tired.
The surgery went well. Patrick woke up and was able to come off the ventilator in no time at all. He was, as always, a favorite with the nurses in post-op. Brian got to reconnect his TPN in post-op, which was kind of funny to do. Our nurse was fascinated with the different equipment. We got some curious looks as Brian drew up vitamins with syringes and injected them into the IV bags.
 It’s a curious thing to be the old pro parents in the hospital. I often refer to myself as a “hospital mom”. We know the routine. We’re patient with the nurses, doctors, and other staff and, although we are concerned for Patrick, we are not scared or intimidated by our surroundings as we once used to be. It’s kind of odd to feel perfectly at home in a hospital… But makes all of this more bearable.
It’s a curious thing to be the old pro parents in the hospital. I often refer to myself as a “hospital mom”. We know the routine. We’re patient with the nurses, doctors, and other staff and, although we are concerned for Patrick, we are not scared or intimidated by our surroundings as we once used to be. It’s kind of odd to feel perfectly at home in a hospital… But makes all of this more bearable.
Patrick was sore and tired for a day and still whimpers if we move his not-quite-healed shoulder the wrong way… But overall he’s back to himself. As for Howie and myself, well, we’re slowly but surely catching up on our sleep and getting back to a normal routine. And preparing for the adventures ahead.
First steps to transplant
And that brings us to the last of the firsts for this entry. We have made the first steps towards transplant evaluation for Patrick. We have appointments for April 27th and 28th at Seattle Children’s Hospital to meet with the surgeon, gastrointerologist and just about anyone else who might have anything at all to do with Patrick’s transplant. Theevalution process is big, long, and very detailed. They want to make sure that Patrick needs and will benefit from a transplant, that he’s healthy enough to have one, and that his home life lends itself to as successful of a recovery as possible. This trip is the first step in that process, and we are excited to go and learn and start building relationships there.
Patrick still has a long way to grow. He’s almost halfway to the 10 kilo weight goal. (He weighs 10 lbs 11 oz.), and so we know this visit won’t end with him on a list. But it’s a start and a step in the right direction.
And so, those are the firsts we have to report for the time being. We’re looking forward to continuing to see him learn and grow. He is so good at using his hands now! And has just started to discover that he has feet. His spirit grows by leaps and bounds every day. Most of all, he amazes us with his incredible patience and optimism.